- Fovea: Small depression in the retina where sharpness is highest. The fovea is located within the center of the macula
- Fundus: The inside, back surface of the eye, which is made up of the retina, macula, optic disc, fovea, and blood vessels
- Intravitreal injection: Form of treatment for diabetic retinopathy in which a medication is injected into the vitreous cavity in the middle of the eye
- Macula: A small area at the center of the retina, which is responsible for central (straight-ahead) vision, the majority of color vision, and the ability to see small details
- Neovascularization: New blood vessels that grow uncontrollably, provoked by a lack of oxygen, which can cause vision loss
- Proliferative diabetic retinopathy (PDR): An advanced stage of diabetic retinopathy in which new abnormal blood vessels and scar tissue form on the surface of the retina; scar tissue can pull on the retina, which can cause retinal detachment and loss of vision
- Retina: Thin layer of nerve tissue that lines the back of the eye; it receives and converts light into electrical signals, which are then sent to the brain by the optic nerve, resulting in sight
- Vitreous: A gel-like substance that fills the inside of the eyeball
References:
American Society of Retina Specialists (ASRS). Diabetic retinopathy. https://www.asrs.org/patients/retinal-diseases/3/diabetic-retinopathy
Turbert D. American Academy of Ophthalmology (AAO). Fundus. 2020. https://www.aao.org/eye-health/anatomy/fundus
Macular Society. What is the macula? 2022. https://www.macularsociety.org/macular-disease/macula/
Blausen.com staff. Medical gallery of Blausen Medical 2014. WikiJournal of Medicine 1. 2014. https://commons.wikimedia.org/wiki/File:Blausen_0389_EyeAnatomy_02.png
All URLs accessed May 27, 2025
![]()
34.2 million people of all ages - or 10.5% of the US population - has diabetes.
![]()
21.4% of people with diabetes do not know they have it.
Reference:
Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2020.
Diabetic retinopathy is a complication of diabetes that causes damage to the blood vessels of the retina — the light-sensitive tissue that lines the back part of the eye. Diabetic retinopathy occurs in more than half the people who develop diabetes and is the most common cause of irreversible blindness in working-age Americans. Despite type 2 diabetes being more common, blindness can affect people with type 1 or type 2 diabetes at similar rates.
It is possible to have diabetic retinopathy for a long time without noticing symptoms until substantial damage has occurred. Symptoms of diabetic retinopathy may occur in one or both eyes.
The primary cause of diabetic retinopathy is diabetes — a condition in which the levels of glucose (sugar) in the blood are too high. Elevated sugar levels from diabetes can damage the small blood vessels that nourish the retina and may, in some cases, block them completely. Damaged blood vessels can leak fluid into the retina, causing swelling of the retinal tissue. Swelling in the macula is called diabetic macular edema (DME), and can affect the sharp, central (straight-ahead) vision needed for activities such as reading and recognizing faces. Prolonged damage to the small blood vessels in the retina results in poor circulation to the retina and macula, causing new, abnormal blood vessels and scar tissue to grow on the surface of the retina. New vessels may bleed into the middle of the eye and cause scar tissue formation, which can pull on the retina and detach it from the back of the eye; these new vessels can also cause high pressure and pain if they grow on the iris, clogging the drainage system of the eye. All of these changes that happen to the eye related to diabetic retinopathy can cause vision loss.
Anyone who has diabetes is at risk of developing diabetic retinopathy. Additional risk factors can include:
- Disease duration: The longer someone has diabetes, the greater the risk of developing diabetic retinopathy
- Poor control of blood sugar levels over time
- High blood pressure
- High cholesterol levels
- Pregnancy
References:
American Society of Retina Specialists (ASRS). Diabetic retinopathy. https://www.asrs.org/patients/retinal-diseases/3/diabetic-retinopathy. Accessed May 27, 2025.
Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2020.
Symptoms of retinopathy may include:
 Blurred or double vision
Blurred or double vision Difficulty reading
Difficulty reading




References:
American Society of Retina Specialists (ASRS). Diabetic retinopathy. https://www.asrs.org/patients/retinal-diseases/3/diabetic-retinopathy
National Eye Institute. Diabetic retinopathy. NIH 2019. https://www.nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/diabetic-retinopathy
Boyd K. Diabetic Retinopathy: Causes, Symptoms, Treatment. https://www.aao.org/eye-health/diseases/what-is-diabetic-retinopathy
All URLs accessed May 27, 2025
The best way to diagnose diabetic retinopathy is a dilated eye exam. During this exam, the physician places drops in the eyes to make the pupils dilate (open widely), allowing a better view of the inside of the eye, especially the retinal tissue.
The physician will look for:
- Swelling in the retina that threatens vision (diabetic macular edema)
- Evidence of poor retina blood vessel circulation (retinal ischemia)
- Abnormal blood vessels that may predict an increased risk of developing new blood vessels
- New blood vessels or scar tissue on the surface of the retina (proliferative diabetic retinopathy)
Regular dilated eye exams by an ophthalmologist are important, especially for those who are at a higher risk for diabetic retinopathy or diabetes. If you are over age 50 years, an exam every 1 to 2 years is a good idea so the physician can look for signs of diabetes or diabetic retinopathy before any vision loss has occurred. If retinopathy is detected, your eye care provider will determine how frequently follow-up exams would be needed and when to refer to a retina specialist.
In addition to this exam, physicians use other tests to detect and manage diabetic retinopathy:
- An optical coherence tomography (OCT) test provides highly detailed images of the layers of the retina that show its thickness, helping to determine whether fluid has leaked into retinal tissue.
- The physician may take photographs of the back of the eye (color fundus photography) to help detect and document diabetic retinopathy. These photos make it easier for the physician to monitor the disease on follow-up visits to determine if it is worsening.
- To evaluate retina blood vessel circulation, a test called fluorescein angiography (FA) may be conducted. After dilating the pupils, the physician will inject a dye into the patient’s arm, which then circulates through the eyes and works like a food coloring; however, it does not affect the kidneys and is unlike the dye that is used with MRIs and CAT scans.
With proper examinations, diabetic retinopathy can be detected before vision loss begins. If signs of diabetic retinopathy are detected, discussions about frequency of follow-up exams and referral to a retina specialist will be important, assisting in the early detection of changes that would need treatment to preserve vision.
Reference:
American Society of Retina Specialists (ASRS). Diabetic retinopathy. https://www.asrs.org/patients/retinal-diseases/3/diabetic-retinopathy. Accessed May 27, 2025.
There are approved treatments for diabetic retinopathy, including intravitreal injections (small injections of medications into the middle cavity of the eye), laser treatments, and vitreous and retina surgery. These procedures can be done in an office or hospital setting to prevent, treat, or reverse damage from diabetes in the retina.
Research has shown that eye injections often result in better vision than laser treatment alone for patients with diabetic macular edema and diabetic retinopathy. The key to these treatments is their ability to block vascular endothelial growth factor (VEGF), a chemical signal that stimulates abnormal blood vessel growth and leakage. Repeated doses of anti-VEGF medications may be needed to prevent blood vessels from leaking fluid and causing vision loss.
Reference:
American Society of Retina Specialists (ASRS). Diabetic retinopathy. https://www.asrs.org/patients/retinal-diseases/3/diabetic-retinopathy. Accessed May 27, 2025.
Even if not all vision loss from diabetic retinopathy can be prevented or treated, patients usually are able to find resources to help them live with diminished vision. If you have been diagnosed with diabetic retinopathy or diabetes and have vision loss that cannot be reversed, a retina specialist can help you find access to rehabilitation with a variety of tools to make everyday living with this disease a little bit easier. A retina specialist can also help connect you with others who have similar limitations.1 (Refer to the RESOURCES section of this website.)
Prevention: Patients with diabetes frequently ask, “Is there anything I can do to keep from getting diabetic retinopathy or to prevent or treat vision loss once it occurs?” If you have diabetes, the National Eye Institute (NEI) suggests that you keep your health on TRACK:1
- Take your medicines as prescribed by your doctor
- Reach and maintain a healthy weight
- Add physical activity to your day
- Control your ABCs — hemoglobin A1c (HbA1c), blood pressure, and cholesterol
- Kick the smoking habit
Regular dilated eye exams reduce the risk of developing more severe complications from the disease.1 Suggested follow-up schedules are listed in the following Table, which may be personalized by your eye care provider depending on the stage of retinopathy and the presence of macular edema.2
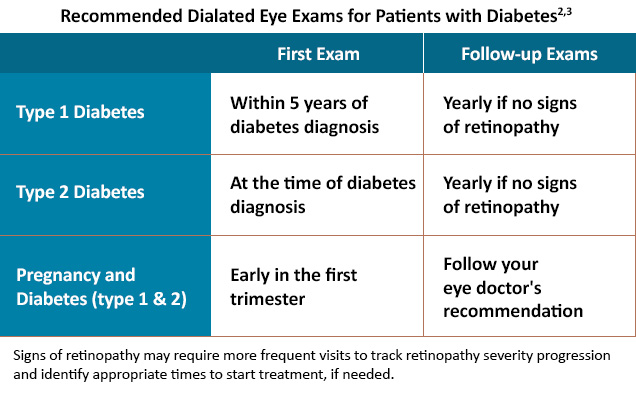
It is extremely important for patients with diabetes to maintain the recommended eye examination schedule, which depends on the severity of disease. Early detection and referral to a retina specialist are essential to starting treatment to prevent vision loss, preserving the activities you most enjoy.1
References:
- American Society of Retina Specialists (ASRS). Diabetic retinopathy. https://www.asrs.org/patients/retinal-diseases/3/diabetic-retinopathy. Accessed May 27, 2025.
- Solomon SD, Chew E, Duh EJ, et al. Diabetic retinopathy: A position statement by the American Diabetes Association. Diabetes Care. 2017;40(3):412-418.
- Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P75-P162.
Some sample questions are listed below to help you begin the conversation with your clinician about your condition.
- Can diabetic retinopathy be prevented?
- What symptoms may I experience?
- If I control my diabetes, will I lower my chances of developing diabetic retinopathy?
- Will I need additional treatment(s) or will taking my diabetes medications be enough?
- If I develop diabetic retinopathy, will I lose my vision?
- If one eye is affected, will the other be automatically affected?
- How often should I see a specialist?
- Is it possible to recover vision lost as a result of diabetic retinopathy?
Use this tool for an easy symptom guide and questions to ask your primary care and eye care providers: Retinopathy Checklist
Taking part in a clinical trial can be a great way to help improve treatment for your eye disease. Your participation can help both you and others who may benefit from the treatment if it is approved by the US Food and Drug Administration in the future. Here are a few things to consider about participating in a clinical trial:
- Ask your eye doctor about clinical trials related to your eye disease.
- If your eye doctor says you may be a good candidate for a clinical trial, don’t be afraid to ask questions about the trial. Some possible questions: What would you need to do to participate? How many visits/appointments are needed related to the trial? Is there any assistance with transportation costs for trial-related appointments?
- If you speak another language, find out if trial-related paperwork is available in your native language.
Before you join the trial, leaders of the clinical trial will let you know what you need to do to participate. They can also let you know how you can leave the trial if you choose to do so. Providing information about the trial and letting you know about any potential treatment side effects is called informed consent.1
For more information about clinical trials, click here to access a variety of educational videos and information about medical research, as well as important questions to ask provided by the US Department of Health and Human Services (HHS).2 Sharing this information with your provider can help you identify appropriate trials for your retinal condition and support discussions on whether or not participation in a clinical trial is right for you.
References
- FDA U.S. Food & Drug Administration. Clinical trial participation. Last reviewed 12/5/2024. https://www.fda.gov/consumers/health-education-resources/clinical-trial-participation
- HHS, Office for Human Research Protections. About research participation. https://www.hhs.gov/ohrp/education-and-outreach/about-research-participation/index.html
All URLs accessed May 27, 2025






{kind=link}